Call today! 614-863-3937
CORNEA TRANSPLANT SURGERY
There are approximately 50,000 Cornea Transplant surgeries performed each year in the United States. This is actually a small number when compared with approximately 5 million cataract procedures each year in this country. Of all transplant surgery done today, including heart, lung and kidney, corneal transplants are by far the most common and successful. Richard A Erdey, MD and Daryl D Kaswinkel, MD are Corneal Specialists; they have been performing Cornea Transplant Surgery since 1988 and 1996 respectively.
View: 10TV News Report
View: Our cornea transplant patient throws out first pitch!
View: testimonials
The Human Eye is like a telescope in that it contains two lenses to focus light onto the retina. The first “lens” is the cornea which is a transparent, dome-shaped structure covering the front of the eye. It is a powerful refracting surface, accounting for 2/3 of the eye’s focusing ability. Because there are no blood vessels in the cornea, it is normally clear and transparent. Like the crystal on a watch, it provides a clear window to look through. To the observer, it glistens due to the constant bathing of tears equally spread onto its surface with each blink of the lids.
The cornea is tough, difficult to penetrate and is extremely sensitive – there are more nerve endings in the cornea than anywhere else in the body. For this reason, a corneal abrasion is generally very painful but fortunately, heals rapidly. The adult cornea is only about 1/2 millimeter thick and is comprised of 5 layers: Epithelium, Bowman’s membrane, Stroma, Descemet’s membrane and the Endothelium. Throughout life the cornea must remain transparent, smooth and of regular curvature to properly transmit and focus light as it enters the eye. Infections, trauma, or dystrophic conditions can involve any layer of the cornea and may result in scarring, thinning or curvature distortion that, if severe, can cause loss of transparency, optical distortion and blindness.
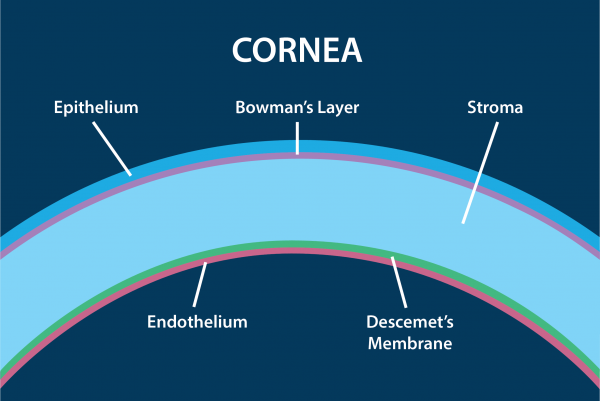
Cross-section of the cornea. The normal cornea is about 0.55 millimeters (mm) thick in its center and consists of five microscopic layers as labeled above. The thickness may increase to 0.68 mm or greater if swelling occurs because of endothelial cell loss.
We are born with a complement of cornea endothelial cells (3000 to 3500 cells/ mm²) that line Descemet’s membrane. These cells are responsible for “pumping” fluid out of the cornea, maintaining cornea transparency. As we mature, the concentration of these specialized cells may decrease by 1/3 but this quantity is still sufficient to maintain corneal clarity throughout life. Unfortunately, corneal endothelial cells are one of the few cells in the human body that are not capable of regeneration and if damaged or lost are not replaced.
If the cornea endothelial cell concentration falls below a certain critical threshold, as can occur in Fuchs’ Corneal Dystrophy, after cataract or cornea transplantation surgery or after eye trauma, the cornea swells and loses transparency leading to blurry vision or eventually, blindness.
Fuchs’ corneal dystrophy is a progressive condition that gradually affects both eyes. It is slightly more prevalent in women than in men. The condition rarely affects vision until people reach their 50s and 60s although an eye doctor can sometimes detect the early signs of Fuchs’ dystrophy at age 30 to 40 years. The pathology in Fuchs’ corneal dystrophy is demonstrated by increasing concentrations of optically degrading tiny dimples which form within descemet’s membrane in between the endothelial cells. The endothelial cells are gradually lost over the years.
At first, a person with Fuchs’ corneal dystrophy may notice subtle deterioration in night vision. As the process progresses, they may awaken with blurry vision that gradually clears later in the morning or later. The reason for this is during sleep the closed eyelids prevent evaporation; once the patient awakens, the open eyelids allow corneal surface evaporation to occur, allowing the cornea to thin and vision to improve. As the disease progresses further, corneal swelling will remain constant and vision remains poor throughout the day.
Eventually, the epithelium also swells with fluid and may form tiny blisters, causing eye irritation, foreign body sensation and severe visual impairment. If these blisters burst they can cause severe pain. These symptoms are also seen with other causes of corneal endothelial failure due to cataract surgery, corneal transplant rejection/late failure, or trauma.
To treat the disease, your doctor may initially try to reduce corneal swelling with hypertonic salt drops or ointment which temporarily extracts the fluid from the cornea. If the condition becomes painful, bandage soft contact lenses may be used. In early stages of this condition, a hair dryer held at arm’s length and directed parallel to face can be used to dry and thin the cornea. This technique may briefly improve symptoms and can be repeated if necessary.
Once the disease interferes with daily activities because visual performance is consistently reduced and/or persistent pain occurs, your doctor may recommend corneal transplantation to restore sight and eliminate discomfort.
There are other conditions of the cornea where the endothelial cells are healthy but the cornea may be scarred, abnormally thinned, warped and distorted. As a result, the light passing through the cornea is not focused as it should. This occurs in advanced Keratoconus, LASIK-induced ectasia (thinning), Radial Keratotomy (RK) induced irregularity, traumatic injury, or various corneal dystrophies.
Corneal Transplantation may be necessary if your cornea is damaged due to injury or disease. Since there is no artificial substitute for corneal tissue, a human donor cornea is transplanted to restore sight. The Central Ohio Lions Eye Bank typically provides the corneal tissue for our patients.
A successful Corneal Transplant requires special, ongoing care and attention on the part of both patient and physician. However, no other surgery has so much to offer when the cornea is deeply scarred or afflicted with disease. View: testimonials
“Don’t take your organs to heaven…heaven knows we need them here! “
Corneal Transplant Surgery would not be possible without the hundreds of thousands of generous donors and their families who have donated corneal tissue so that others may see. If you would like more information on becoming a donor, please contact the Central Ohio Lions Eye Bank at (614) 293-8114 or (800) 301-4960
Drs. Erdey and Kaswinkel may recommend one of the following surgical variations of corneal transplantation at the time of your consultation:
Penetrating Keratoplasty (PK) is a traditional full-thickness corneal transplant. This may be required in cases where the cornea is scarred, swollen or excessively thin (Keratoconus).
Return of best vision after standard full thickness corneal transplantation may take up to a year or more after the operation. It is dependent on how long it takes for the grafted cornea to begin functioning as a lens; it must become transparent and it must have a regular surface curve. These important characteristics permit light to properly bend (refract) as it passes through the cornea, bending further as it passes through the crystalline lens and comes to focus on the retina.
The newly grafted cornea, if successful, only takes a few weeks to become thin and transparent but far more time is usually required until light is properly refracted through it.
The healthy cornea is transparent because it does not contain the fine blood vessels (capillaries) present in other tissues of the body. However, this lack of blood supply has a downside when cornea graft wound-healing is required. The cornea takes years to heal as compared to a superficial wound in the skin of your arm, which heals in only about a week! For this reason cornea graft sutures must be left in place for a year or more while the cornea graft-host interface heals. The tension generated by the sutures within the cornea often cause distortion of the curvature of the graft, causing the refraction of the eye to shift unpredictably. If the cornea surface is regular, and the prescription of the other eye is not too different, it is sometimes possible to prescribe glasses during this early rehabilitation period but the prescription lenses may need to be periodically changed as the cornea heals.
Some patients may need to wait until the sutures can be removed (1 to 1.5yrs) before the final surface topography is apparent and then glasses are prescribed. However, if after suture removal, significant cornea graft distortion or warpage (irregular astigmatism) remains, spectacles will not help. Instead, hard contact lenses may be suggested, but fitting can be challenging and is not always successful.
Other individuals require laser vision correction to reduce inadequate graft curvature or imbalances between the prescriptions of both eyes to maximize optical visual rehabilitation.
Of course, a good visual outcome is also dependent on general eye health and requires the absence of other visually limiting conditions such as cataract, glaucoma, or macular degeneration.
Deep Anterior Lamellar Keratoplasty (DALK) is an elegant partial thickness graft that unlike full-thickness corneal transplatation (PK), preserves the TWO inner most layers of the cornea: Descemet’s membrane and the endothelium, while removing and replacing only the diseased, weakened or scarred anterior layers with donor tissue. If the endothelial layer is normal, then its preservation is important. Why?...because unlike most cells in the body, endothelial cells do NOT replicate if lost or damaged. What's worse...donor corneal endothelial cells do NOT have the same longevity as your own! After 5 years, donor median endothelial cell counts on a PK graft decay by about 70%. This means if you start out with 2700 cells/mm(2) on a donor cornea, after only 5 years you might expect to only have 810 cells/mm(2). A minimum of about 600 cells/mm(2) are required to pump fluid out of the cornea and maintain it's transparency. If an endothelial cell graft rejection occurs during this same period, the loss may be accelerated and the graft could fail (become swollen and opacified requiring a regraft). - the cornea swells like a dry sponge with water added.
DALK: Cross section of cornea showing partial thickness cornea graft. Note: Descemet’s membrane and endothelial cell layer is retained and NOT replaced.
Retention of this important layer not only eliminates endothelial cell rejection preserving endothelial cell density so the graft should last a lifetime, but also makes the creation of larger diameter grafts possible. Since 2007, Drs. Erdey and Kaswinkel have refined techniques which permit the creation of larger diameter DALK grafts which tend to have less astigmatism, less optical aberration and are associated with more rapid optical rehabilitation than smaller diameter DALK grafts. The final suture-out topography is stable and maintains its shape over time making it closer to a true "refractive surgical procedure"! These superior visual outcomes and a DALK graft that should not have to be repeated due to endothelial cell exhaustion or rejection have marginalized PK in our practice - to only those few corneas with full-thickness severe pathology or PK ectasia or graft failure.
Read: Large-diameter DALK technique minimizes post-operative astigmatism - Richard A. Erdey, M.D.
Very few cornea specialists offer DALK as it is an extremely delicate, time intensive and poorly reimbursed procedure despite it’s many benefits. In 2016, in the USA, only 1232 DALK’s were performed in contrast to 20,000 eyes that had PK, full-thickness, traditional corneal transplants when the majority of these would have been suitable DALK candidates. By 2021, the number of domestic DALK procedures dropped to only 544 (EBAA Annual report 2021). Drs. Erdey and Kaswinkel perform a very significant % of our country's DALK procedures and nearly 100% of the larger diameter DALK.
Dr Erdey frequently speaks and teaches at local and national conferences to his colleagues in an effort to reduce the barriers to surgeon acceptance. He passionately believes broader surgeon acceptance and conversion from PK to DALK needs to occur on a wider scale.
 |
Cornea after DALK: donor graft applied to retained recipient descemet’s membrane. Cornea transparency is restored. Sutures generally removed after 6 mos. |
The most suitable candidates for this procedure include those who are not suitable cornea cross linking or INTACS candidates and otherwise have healthy cornea endothelium, minimal descemet’s membrane scarring are gas permeable hard/scleral contact lens intolerant and who have advanced corneal ectasia (cornea warpage, thinning with or without scarring) from:
» Keratoconus
» Keratoglobus
» Corneal Hydrops
» Pellucid Marginal Degeneration
» LASIK or PRK complications
» Radial Keratotomy (RK) complications
or who have other conditions such as:
» cornea scarring due to cornea dystrophies, prior infection or trauma
» cornea melting due to exposure or autoimmune conditions
» active infectious keratitis unresponsive to medication
Advantages:
» Closed eye surgery
» No chance of potentially blinding endothelial rejection because the recipients own descemet’s membrane and endothelial cell layer is retained
» Can potentially repeat DALK or perform PK if the results of the original procedure are not satisfactory
» Better control of post-operative astigmatism particularly when large diameter grafts used.
Disadvantages:
» Conversion to full thickness PK may be required if perforation of descemet’s membrane - only 0.018 mm thick, about the thickness of cellophane, but not nearly as strong! Since 2010, Dr Erdey and Kaswinkel's combined success rate of retaining host descemet's membrane when DALK is attempted, is over 99%!
» Irregular astigmatism far less common than PK but still possible
» Technically challenging
» Significantly longer operative time
» Offered by few cornea surgeons
Innovations:
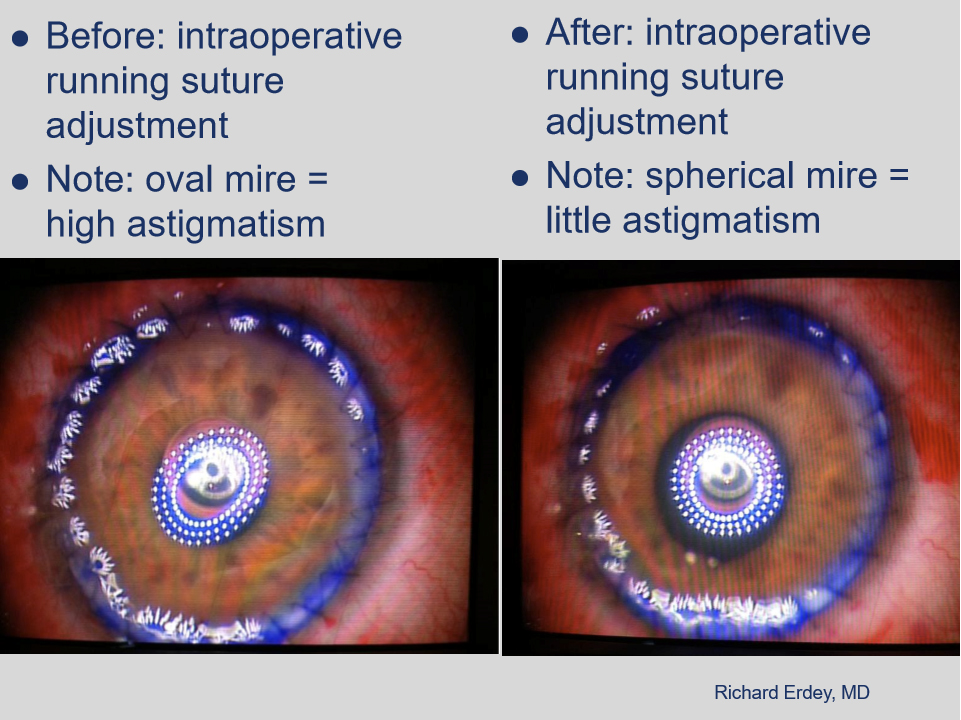
Mastel Intraoperative Keratometer allows cornea graft running suture adjustment - reduces astigmatism and allows for rapid visual rehabilitation

View: Dr. Erdey’s case studies utilizing large (9.5-10mm) DALK to achieve rapid restoration of natural corneal curvature and transparency:
View: Testimonial: DALK for Radial Keratotomy (RK) ectasia Case #4
Descemet’s Membrane Endothelial Keratoplasty (DMEK) and (DSEK) are cornea-sparing transplant procedures of the posterior layer of the cornea indicated for patients without corneal scarring and with disease limited to the innermost corneal layer (endothelium) such as Fuchs’ Endothelial Dystrophy or Pseudophakic Bullous Keratopathy.
| DMEK: Cross Section of Cornea showing partial thickness posterior donor layer replaced on undersurface of a patient’s cornea after posterior diseased portion stripped off. |
Only the inner cornea layer is transplanted, leaving the patient’s cornea mostly intact. A small scleral incision is made and few sutures are required. The cornea heals very quickly and is less susceptible to injury or rupture as compared to standard PK. Visual recovery is much faster since the cornea’s original curvature is essentially unchanged resulting in little refractive shift. In contrast, after standard PK, patients often experience large changes in the amount of nearsightedness, farsightedness, and astigmatism. We no longer recommend traditional PK for suitable candidates with Fuchs’ Endothelial Dystrophy or Pseudophakic Bullous Keratopathy.
In 2006, Dr Erdey brought Descemet's Stripping Endothelial Keratoplasty (DSEK) to Central Ohio and in 2010, Dr Erdey became the first in Ohio to routinely perform newer variations of DSEK called Descemet’s Membrane Endothelial Keraoplasty (DMEK). These variations require specially prepared cornea tissue from highly trained eye bank technicians. In 2011, with Dr. Erdey’s encouragement, Central Ohio Lions Eye Bank became only the second eye bank in the U.S. to offer this preparation! Drs. Erdey and Kaswinkel continue to refine, and currently prefer DMEK over DSEK in most cases, because of the higher probability of superior visual results. Also, In a recent study, the incidence of cornea rejection two years after DMEK surgery was 15x less compared to DSEK and 20x less compared to PK.
 |
| Case 1: Cornea after DSEK: donor disc applied to inner cornea surface adds thickness due to retained donor stroma (note step-up - opaque wedge). Cornea transparency is restored. |
 |
| Case 2: Cornea after DMEK: Cornea transparency and anatomy is restored to natural condition without adding additional thickness as in DSEK. |
As in any kind of surgery, many different complications can occur. One unique to corneal transplantation is rejection of the donated tissue. Cornea transplants are rejected five to 30 percent of the time and can occur any time after cornea transplantation. The rejected cornea clouds and vision deteriorates. The warning signs of cornea graft rejection are RSVP:
» Redness – graft rejection may be associated with a red eye
» Sensitivity – to light, any increase from your baseline
» Vision – decrease in vision, especially if foggy or cloudy
» Pain – discomfort, irritation or foreign body sensation
If YOU ARE EXPERIENCING ANY ONE OF THESE WARNING SIGNS, YOU MUST IMMEDIATELY CONTACT YOUR OPHTHALMOLOGIST AND SCHEDULE AN APPOINTMENT TO BE SEEN WITHIN 24 HOURS, EVEN IF MANY YEARS HAVE PASSED SINCE THE ORIGINAL CORNEA TRANSPLANT SURGERY!
Most rejections, if detected and treated promptly, can be reversed with minimal injury.
CORNEA GRAFT REJECTION HANDOUT:
All cornea transplant patients are required to print, read and keep this document for future reference.
Never discard this important document! Be informed! If the transplanted cornea fails, the graft may be replaced with a new donor, usually with good results, but the overall rejection rates for repeated transplants are higher than for the first transplant.
Other possible complications listed below can usually be treated and include:
» infection
» bleeding
» retina swelling or detachment
» glaucoma
» irregular astigmatism
After uncomplicated Corneal Transplantation, vision may continue to improve up to a year or more after surgery. If the surgery is successful, other existing eye conditions, such as macular degeneration, glaucoma, or diabetic retinopathy, may limit vision after surgery. Even with such problems, a corneal transplant may still be worthwhile.
Various Stem Cell Research projects may hold the promise of finding ways to stimulate corneal endothelial cell regeneration. This is the “holy grail” that could eventually eliminate cornea transplantation in cases of endothelial cell loss. Other research is dedicated to developing better artificial corneas or eventually regenerating entire living corneas for transplantation.
icanseeclearly.com – Cornea Transplantation PK, DALK, DSEK, DMEK, DMAEK Columbus, Ohio